Health in Aweil
Health in Aweil

Fox Health Facility - Nyalath Payam
On this page
This data and analysis are based on the Community-based Assessment of Reintegration and Absorption Capacity in Northern Bahr el Ghazal (NBeG), South Sudan (December 2024). The assessment examines the integration status of displaced and returned households living in NBeG, Aweil Central, North, West and East counties, and evaluates the area’s capacity to welcome additional arrivals.
What is the health policy environment?
The South Sudan National Health Policy 2016 – 2026 focuses on universal health services coverage for all communities through effective, affordable, and comprehensive delivery of health service packages. However, the national public health policy does not disaggregate beneficiaries, including refugees and asylum seekers.
Paragraph 33(g) of the 2012 Refugee Act provides that refugees shall be entitled to the same essential health services as those received by nationals.
What health infrastructure and services are available in Aweil?
The infrastructure assessment profiled 40 healthcare facilities across Aweil and the surrounding areas. While a significant number of facilities were assessed to be in good condition, others, particularly in rural areas, are in poor or very poor condition, highlighting disparities in resource allocation and maintenance.
Healthcare facilities in NBeG are present but strained. Access to essential medicines, such as antibiotics, is inconsistent, while specialized care, including maternal health and mental health services, is severely limited. Staffing remains low, especially for trained professionals, forcing facilities to rely on underqualified personnel. Costs of treatment and long travel distances further hinder access, particularly for returnees.
What are the national standards?
The assessment categorised health facilities based on their service capacity thresholds, based on with national Government and international Sphere Standards. These thresholds define the number of people a facility can reasonably serve under varying conditions.
Health Facility type | Service capacity thresholds |
Primary Health Care Units (PHCUs) and Primary Health Care Centre (PHCCs) | Ideal capacity: 10, 000 people per facility |
Strained Capacity: 25,000 people per facility | |
Maximum Capacity: 50,000 people per facility | |
| County District hospitals | Ideal capacity: 50,000 people per facility |
Strained capacity: 250,000 people per facility | |
Maximum capacity: 300,000 people per facility |
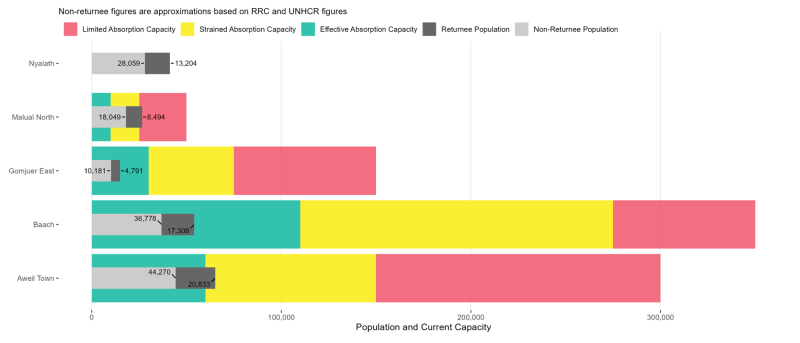
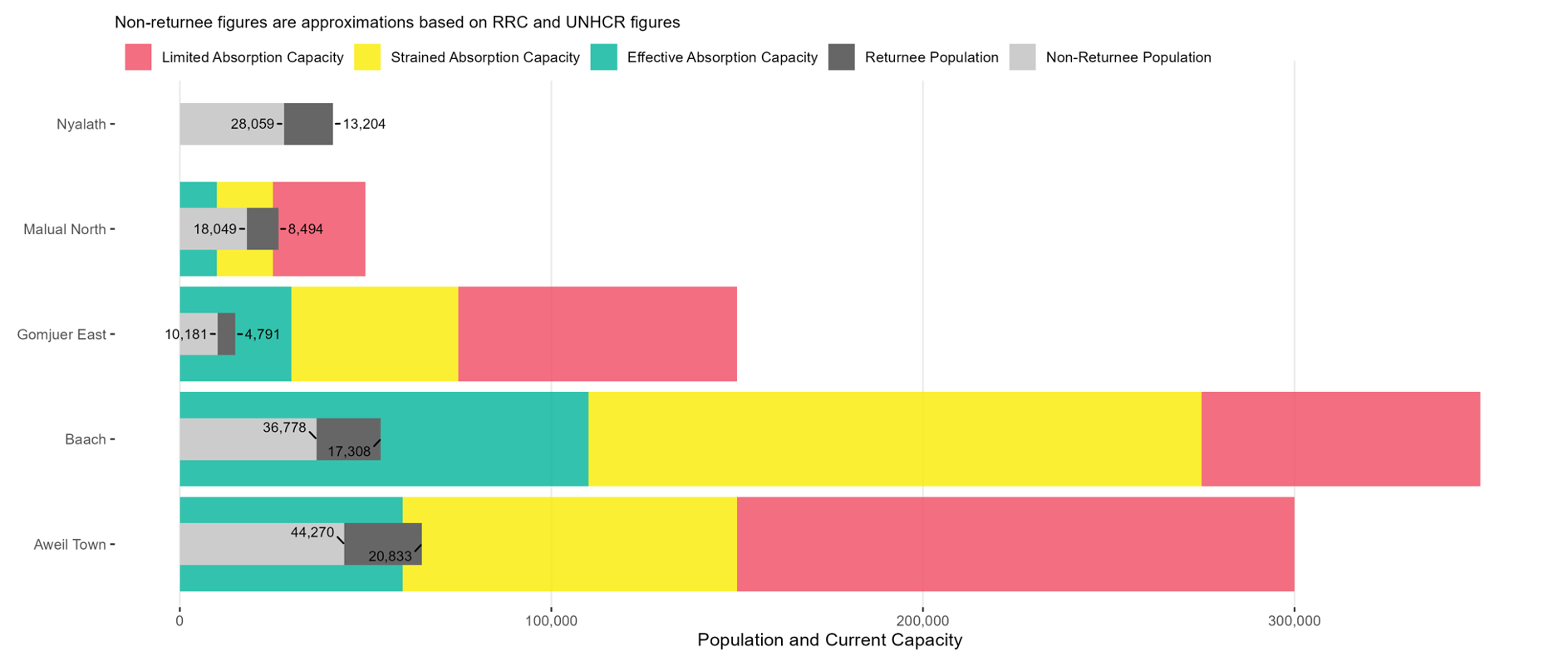
What is the health service absorption capacity?
The healthcare system in the area shows significant disparities in its ability to absorb additional populations. While regions like Gomjuer East and Baac remain within manageable service limits, others, such as Malual North and Nyalath, have already exceeded maximum capacity thresholds. Nyalath, in particular, lacks a single functioning facility that meets minimum quality standards. Across the assessed locations, 28 of the 40 healthcare facilities failed to meet basic standards due to inadequate water access, limited medicine stocks, and poor infrastructure.
Of the 40 healthcare facilities mapped across the region, 28 (65%) did not meet the minimum quality standards to meaningfully contribute to absorption capacity. Health facilities in Nyalath stand out because no facilities that met the minimum quality standards were observed to meaningfully contribute to absorption capacity. For most health facilities, the stock of medicines was identified as the primary issue, affecting 53% of these poor-quality facilities’ contribution to the region’s absorption capacity.
{kind=link}
What is the quality of health facilities?
Based on quality scoring metrics, health facilities scored 56 out of 100 in Northern Bahr el Ghazal given aggregated scores on several indicators. Facilities in this location scored well across the indicators for safety, cleanliness, building condition and having a daily doctor patient ratio which meets national standards. However, the facilities scored under 50 on a variety of important indicators, including availability of medical equipment, supplies and essential medicines, variety of services offered and employment of female medical personnel. These findings highlight that while capacity of healthcare infrastructure is at an effective level given the quantity of facilities functioning at a base level, significant quality concerns remain.
What are the recommendations and priority investments?
Despite an overall effective absorption rate, regional disparities persist. In Nyalath payam, no facilities meet minimum standards, leaving 41,000 people without local healthcare. Refurbishing two centres with water access, toilets, and essential medicines would enable this location to meet a strained capacity, but three additional health centres are needed for ideal service. Across the region, healthcare quality is poor, with facilities scoring under 50% on key indicators like equipment, medicines, service variety, and female medical staff. To improve healthcare in Northern Bahr el Ghazal, prioritising equipment distribution and expanding specialized care is essential.
The estimated number of facilities (refurbished or built) required to fill that gap for each payam is presented in the table below
| Aweil Town | Baac | Gomjuer East | Malual North | Nyalath | |
| Number of working facilities (Dec 2024) | 6 | 2 | 3 | 1 | 0 |
| Number of non-functional facilities (Dec 2024) | 13 | 6 | 1 | 5 | 3 |
| Number of Primary Health Care Units (PHCUs) required to meet ideal service provision and effective absorption capacity | 2 | 0 | 0 | 3 | 5 |
| Number of PHCUs required to meet strained service provision and absorption capacity | 0 | 0 | 0 | 1 | 2 |
| Number of PHCUs required to meet maximum service provision and limited absorption capacity | 0 | 0 | 0 | 0 | 1 |